Screenshot_6-8-2025_114056_gateway.medicalboard.georgia.gov_.jpeg
An official website of the State of Georgia.
The .gov means it’s official.
Local, state, and federal government websites often end in .gov. State of Georgia government websites and email systems use “georgia.gov” or “ga.gov” at the end of the address. Before sharing sensitive or personal information, make sure you’re on an official state website.
Still not sure?
Call 1-800-GEORGIA to verify that a website is an official website of the State of Georgia.
How Do I …
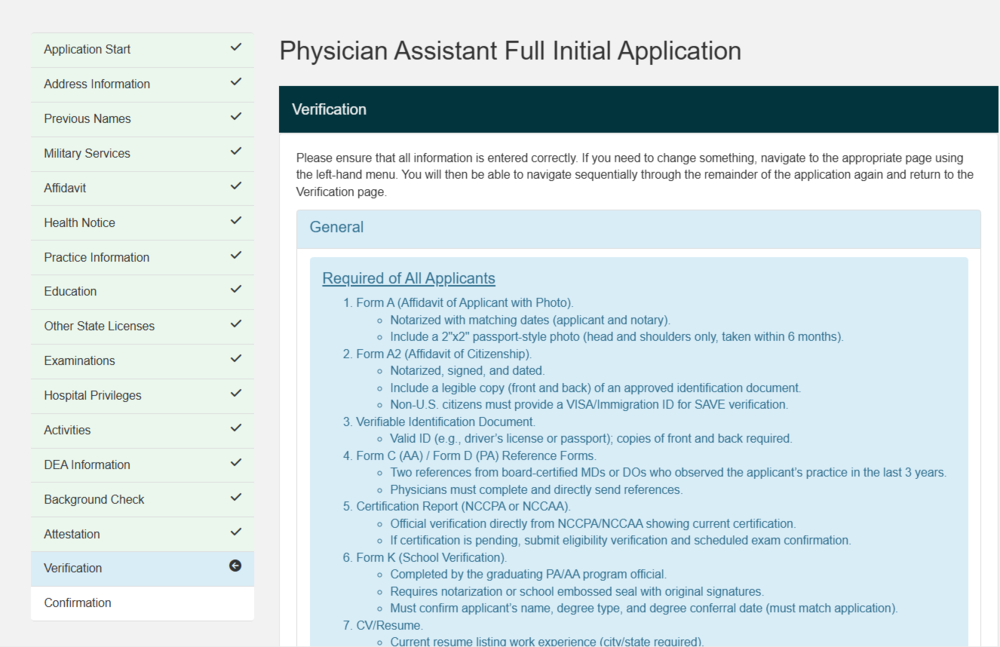
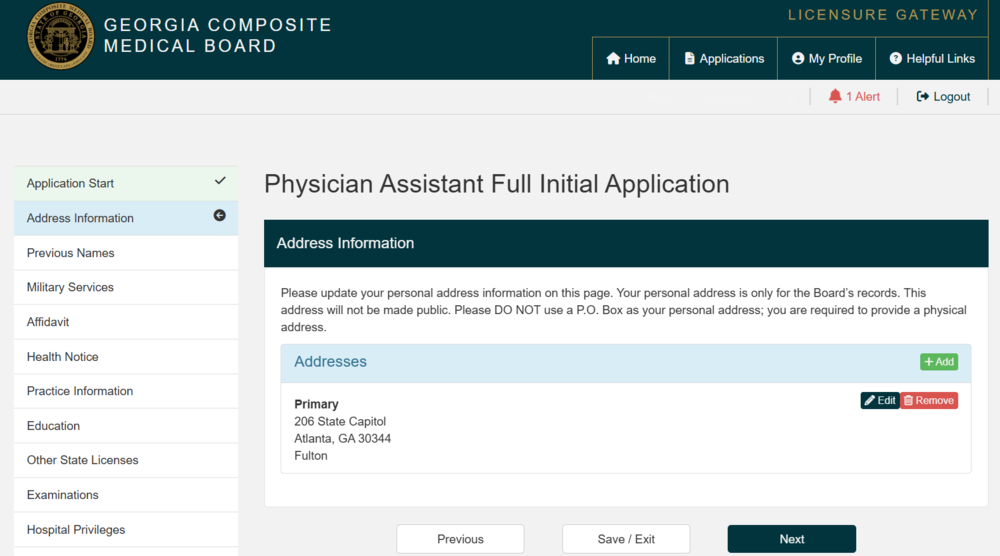
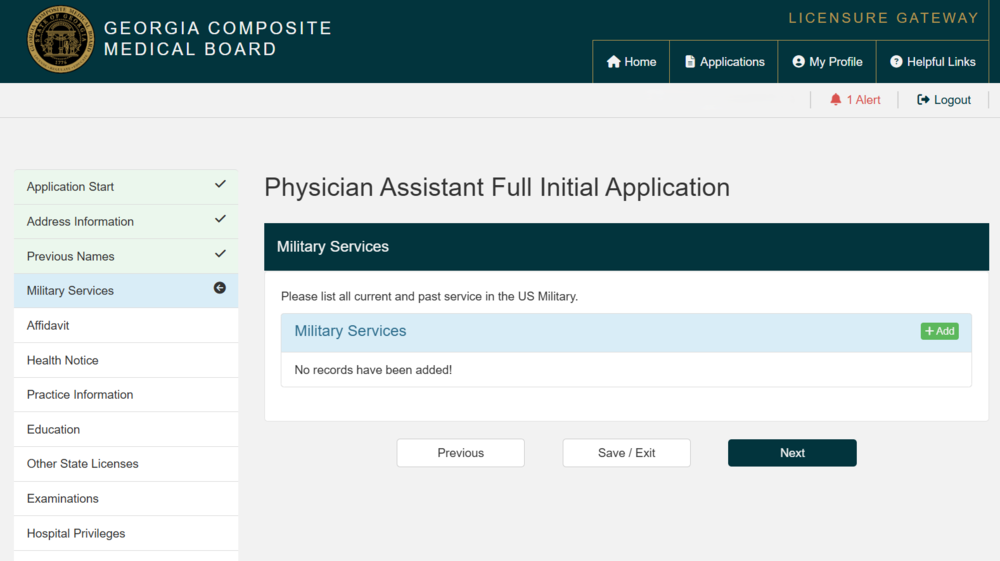
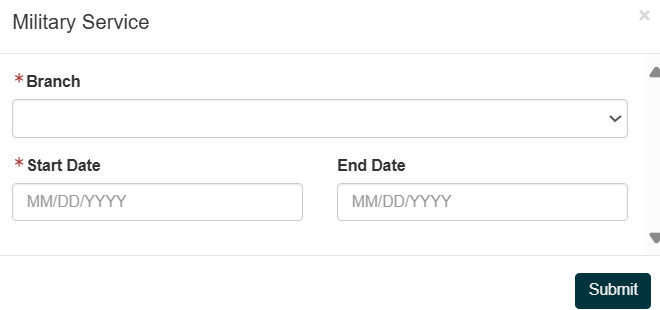
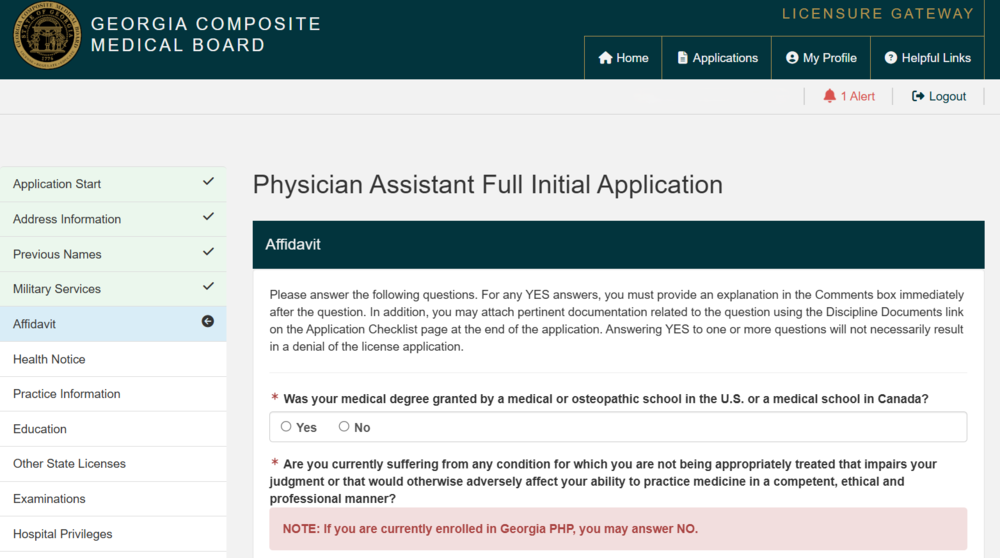
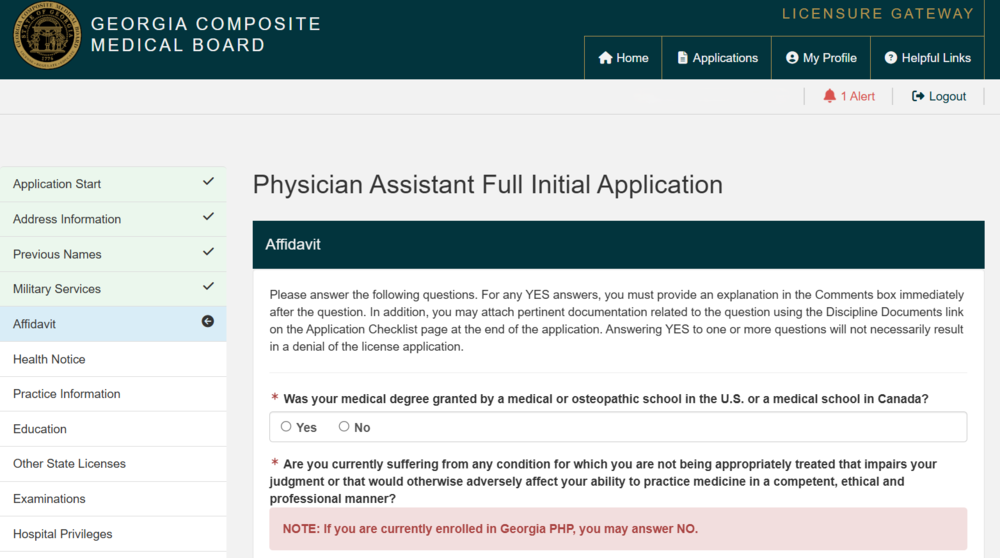
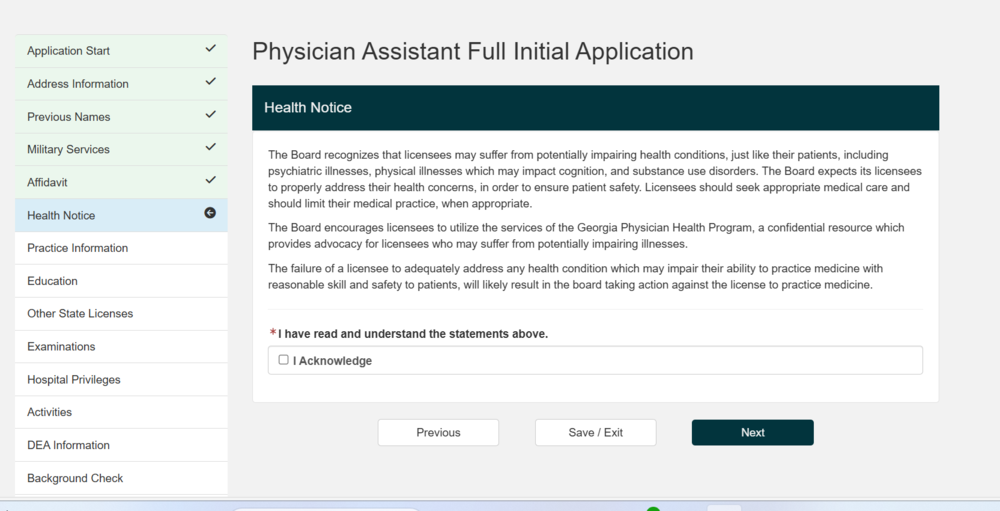
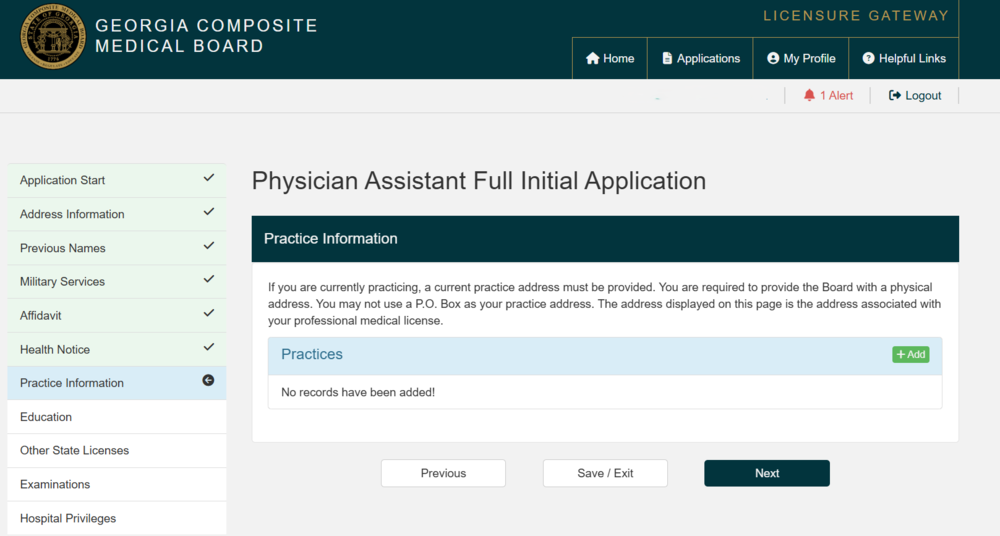
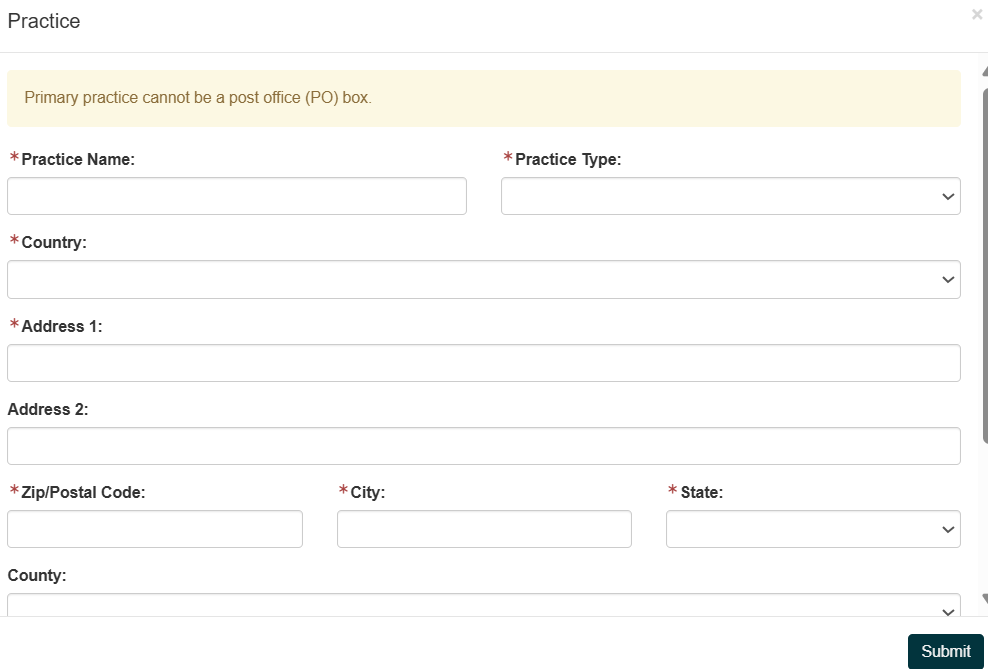
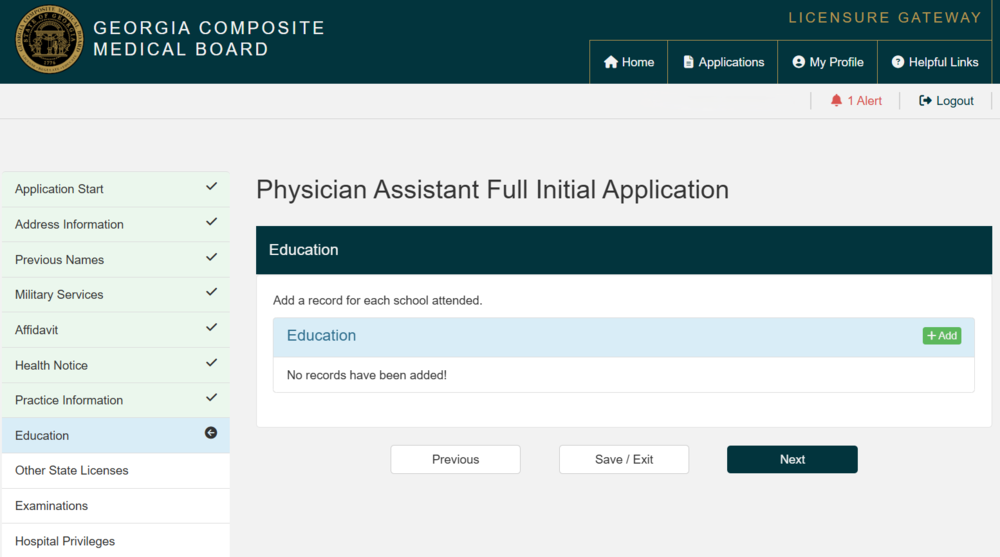
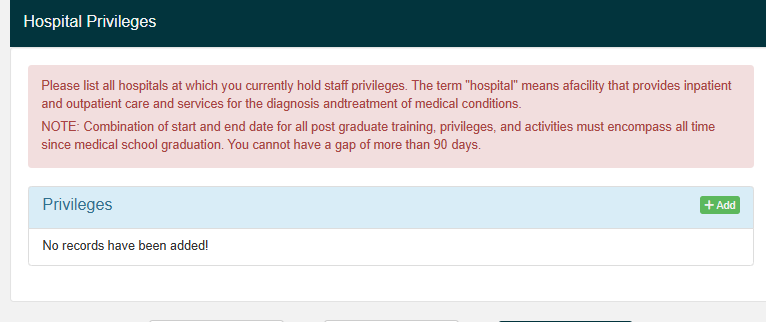
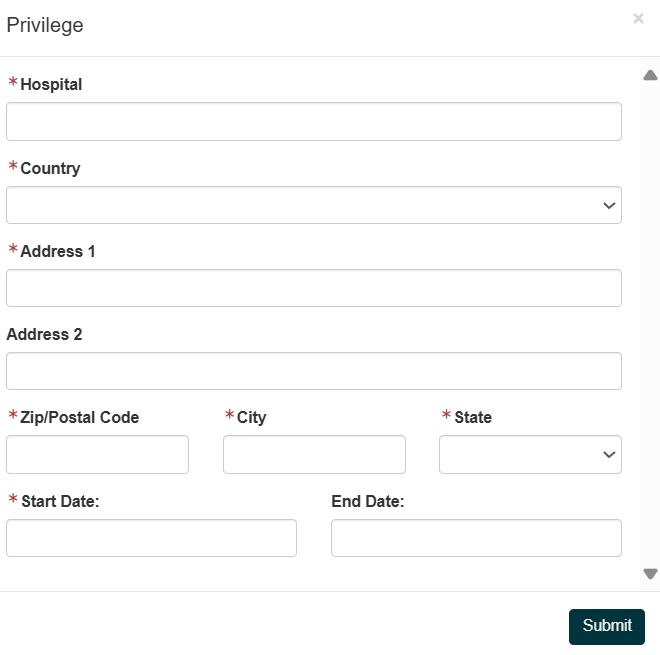
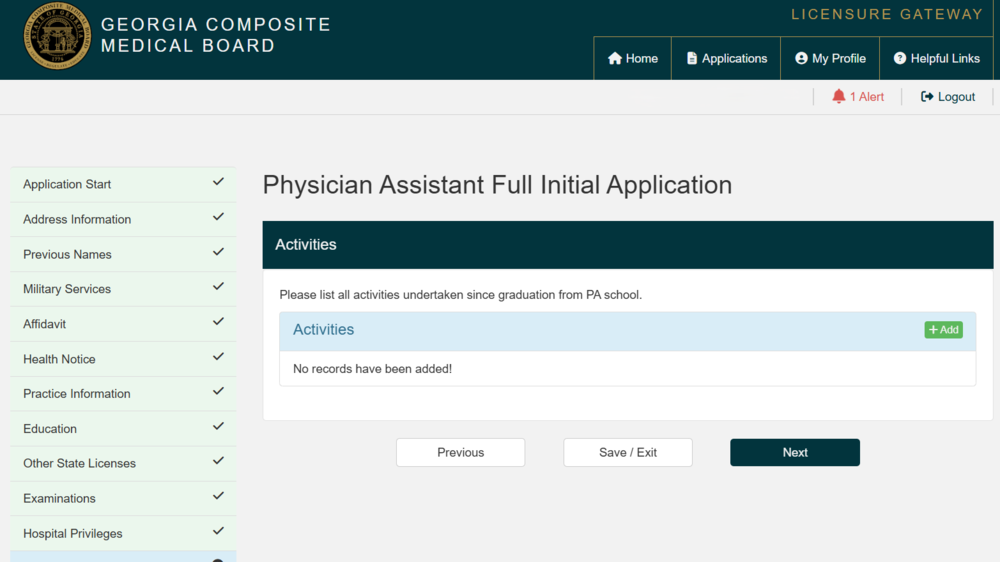
Below is a comprehensive, step-by-step, evidence-driven guide on how to fill out a Physician Assistant (PA) Full Initial Application with the Georgia Composite Medical Board. This guide excludes the "Required Documents" checklist portion and focuses solely on the step-by-step data entry, form completion, and attestation process shown in the application workflow.
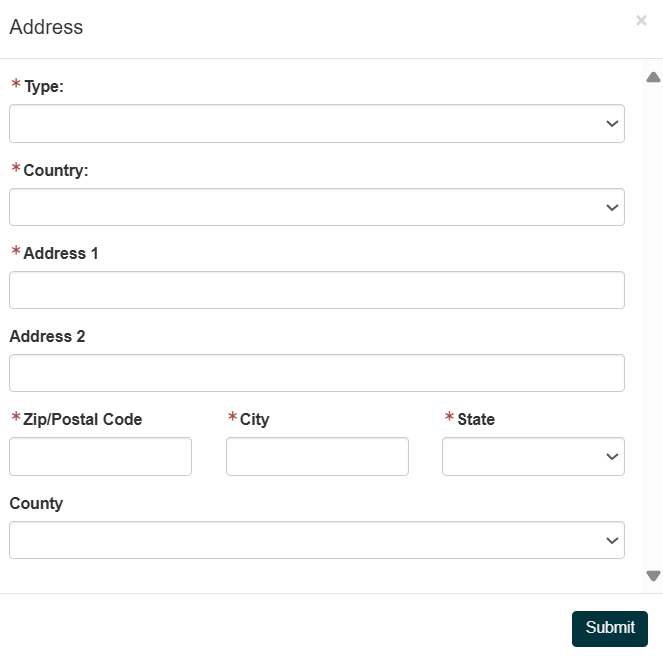
Personal Address:
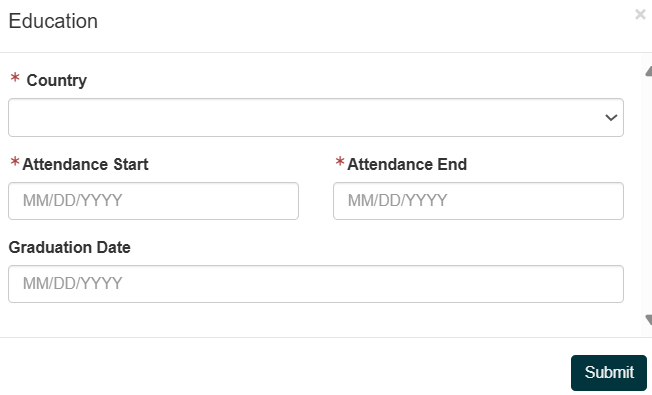
Add a record for each educational institution attended.
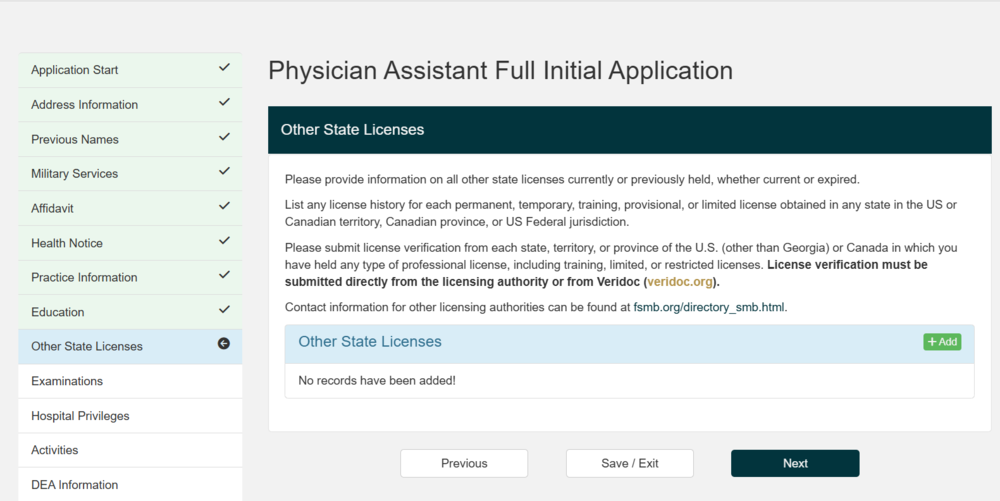
List all current or prior licenses held in any U.S. state or Canadian province/territory (including training, temporary, provisional, limited, and full licenses).
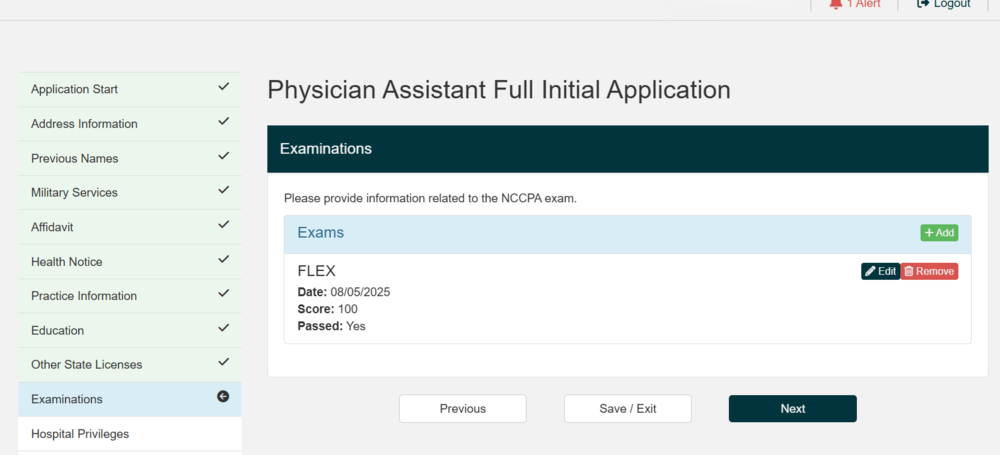
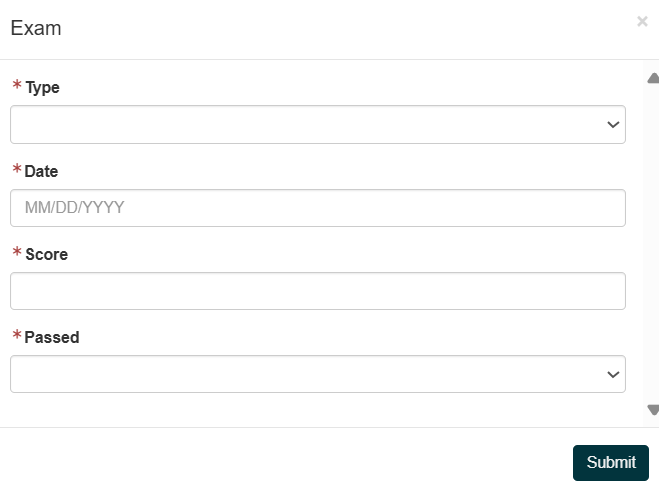
Enter all relevant examination information (typically NCCPA for PAs).
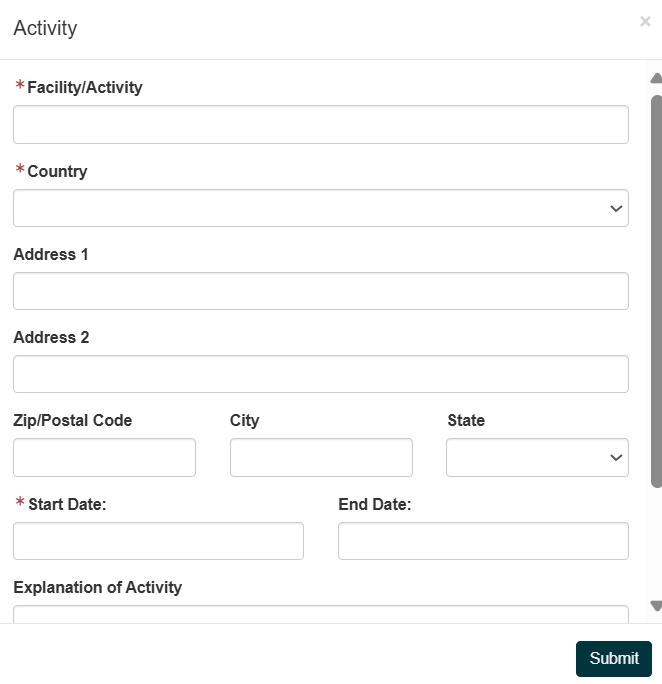
List all professional activities since PA school graduation.
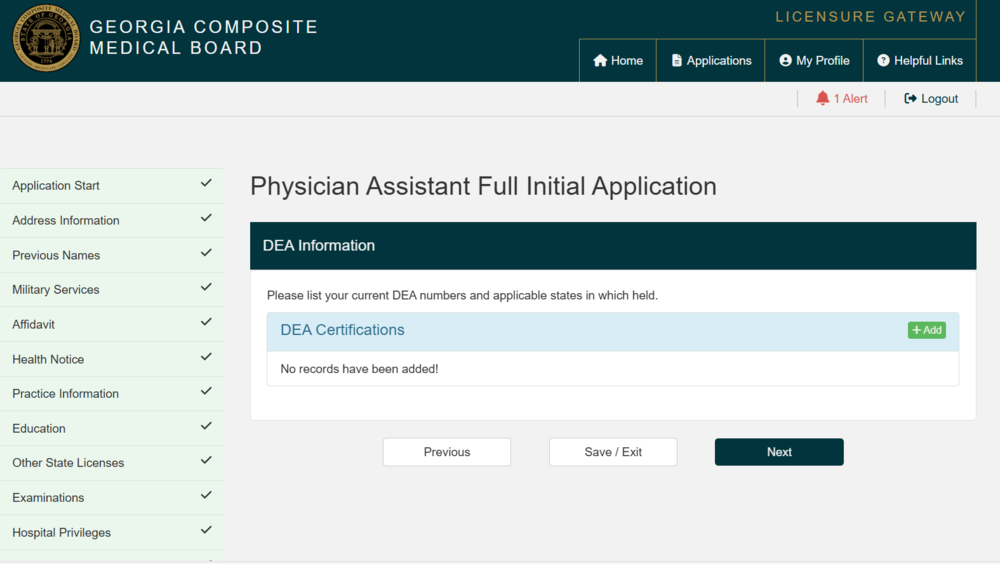
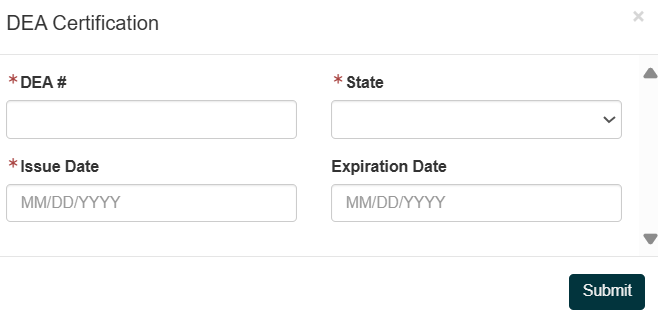
If you hold or have held a DEA registration, enter all current DEA numbers and the states in which they were issued.